ASBM Urges Congress to Support EPIC Act: Remove IRA’s “Pill Penalty” to Ensure Continued R&D for Small-Molecule Drugs
March 5, 2025
On February 25th, the House of Representatives introduced the Ensuring Pathways to Innovative Cures (EPIC) Act (H.R. 1492) an important step toward fixing the Inflation Reduction Act’s (IRA) small molecule pill penalty. Small-molecule drugs typically come in pill or tablet form, and comprise 90% of prescriptions filled in the U.S. The Senate introduced its companion bill, S. 832, on March 4th. In response, ASBM released a statement urging legislators in both chambers to support the EPIC Act.
Under the Inflation Reduction Act (IRA), small-molecule drugs, which account for more than 90% of all prescriptions and typically come in pill form, are subjected to price control mechanisms just nine years after their market introduction. In contrast, biologic medicines—complex treatments administered via injections or infusions—are not subjected to price negotiations until 13 years post-launch. This disparity discourages investment in small-molecule drug research, as manufacturers have a shorter period to recoup their research and development costs. Since the implementation of the IRA in 2021, investment in small-molecule drug development has plummeted by 70% as manufacturers shift resources toward biologics. From ASBM’s statement:
“The ‘pill penalty’ imposed by the IRA has severely curtailed investment in small-molecule drug research,” stated Michael Reilly, Executive Director of ASBM and former Associate Deputy Secretary in the U.S. Department of Health and Human Services. “Small molecule drugs are critical for the treatment of many serious conditions like heart disease, cancer, and mental health disorders. This ‘pill penalty’ jeopardizes the health of millions of patients today and in the future as new small molecule treatments aren’t developed. The EPIC Act is a crucial step in ensuring that American patients continue to have access to innovative therapies for these and other conditions.”
Read ASBM’s statement supporting the EPIC Act here.
View a Fact Sheet on the “Pill Penalty” developed by ASBM Member We Work For Health here.
Learn more about how the IRA affects patients at ASBM’s microsite IRAPatientInfo.org
——
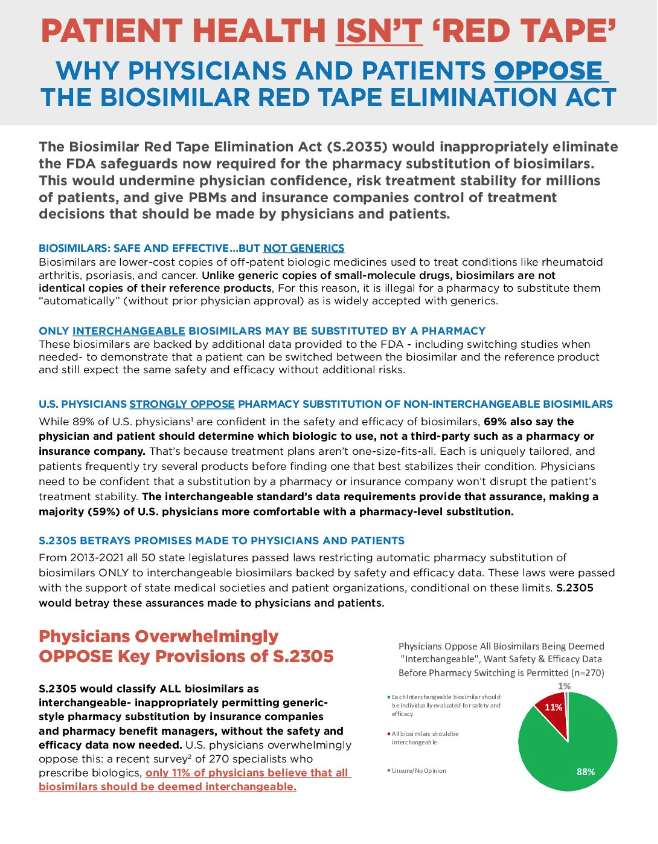 From the Fact Sheet: U.S. Physicians Strongly Oppose Pharmacy Substitution of Non-Interchangeable Biosimilars
From the Fact Sheet: U.S. Physicians Strongly Oppose Pharmacy Substitution of Non-Interchangeable Biosimilars